If you manage or oversee a substance use treatment program, you already know this: great clinical care doesn’t always translate into clean claims. More often than not, it’s not the service itself that causes billing delays or denials but the documentation behind it.
At Integrity Billing, we work with behavioral health facilities every day, and we see the same documentation issues come up again and again. They’re rarely intentional, but they can quietly disrupt cash flow, increase rework, and create frustration for both clinical and billing teams.
Here are three of the most common documentation problems that interfere with substance use billing and what you can do to stay ahead of them.
1. Missing or Incomplete Signatures
This one seems simple, but it’s one of the biggest claim stoppers.
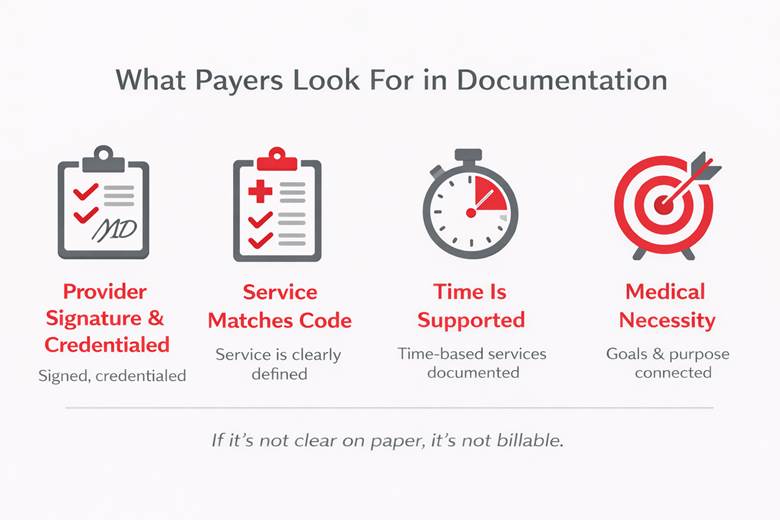
Payers typically require that clinical notes, treatment plans, and evaluations be signed and dated by a provider whose credentials meet their credentialing and contracting standards. When a signature is missing, illegible, or doesn’t include credentials, claims are often denied outright.
Common scenarios we see include:
- Notes saved but never signed
- Group notes missing a facilitator signature
- Credentials not listed after the provider’s name
- Late signatures added after claims are already submitted
From a substance use billing standpoint, unsigned documentation is considered incomplete documentation. This is the case because payers view signatures as proof the service actually occurred and was provided by a qualified professional. Without that, reimbursement is at risk.
A quick review before claims go out can save weeks of back-and-forth after. Integrity Billing recommends building signature checks into your daily or weekly workflow, using EHR alerts or reports to flag unsigned notes, and training staff on signature expectations, including credentials.
2. Services Don’t Match the Documentation
Another common issue is when what’s billed doesn’t clearly line up with what’s documented.
For example:
- A claim is billed for individual therapy, but the note reads like a case management session
- A group therapy code is used, but the note lacks group content or interaction details
- Time-based codes are billed without enough time documented
- The service sounds supportive, but not therapeutic
Even small wording choices can make a big difference. Payers are looking for documentation that clearly supports the type, intensity, and purpose of the service billed. If auditors or reviewers can’t tell from the note why a specific code was used, they’re likely to downcode, deny, or request refunds later.
Your notes should tell the same story your claims are telling. Make sure all documentation aligns with billed services, train clinicians on how to document to the level of care and code, and encourage clear language that reflects medical necessity and treatment goals.
3. Gaps in Medical Necessity and Treatment Planning
Even when notes are thorough, claims can still be denied if medical necessity isn’t clearly supported across the record. At Integrity Billing, we often see progress notes that don’t connect back to the treatment plan, notes that describe activity but not clinical purpose, and treatment plans that aren’t updated as the client progresses.
Payers want to see a consistent story. They look for why the client needs services, what they’re working on, and how treatment is helping. If that connection isn’t obvious, claims are vulnerable. In fact, medical necessity is one of the top reasons for behavioral health denials. Without it, even perfectly coded claims can fail.
To maintain strong documentation, regularly review and update treatment plans, use language that explains clinical reasoning (not just activities), and reference goals and progress in treatment notes. In other words, don’t just describe what happened but why it mattered.
Why These Issues Keep Coming Up
In busy treatment settings, documentation often happens at the end of long days. Staff are balancing client care, crises, groups, intakes, and discharges, and notes can feel like one more thing on the list.
But from a revenue cycle perspective, documentation is the foundation. When it’s incomplete or unclear, billing teams are left trying to fix problems after the fact, and that’s where delays, denials, and lost revenue creep in.
Partnering with a substance use billing company like Integrity Billing is the answer to these issues. We don’t just submit claims—we partner with behavioral health facilities to identify documentation trends that impact reimbursement. Our team helps:
- Flag recurring issues before they become patterns
- Provide feedback on payer expectations
- Improve communication between clinical and billing staff
- Reduce rework, denials, and payment delays
Strengthening Documentation to Protect Your Revenue
Documentation doesn’t have to be perfect to be effective, but it does need to tell a clear, complete story. By addressing common issues like missing signatures, mismatched services, and weak medical necessity, facilities can dramatically improve their billing outcomes.
If your organization is struggling with unexplained denials, slow payments, or recurring documentation issues, it may be time for a deeper look.
Integrity Billing offers a free forensic billing assessment to help facilities uncover documentation gaps, coding risks, and process breakdowns that may be impacting revenue. There’s no obligation—just clear insight into where improvements can make the biggest difference.
Fill out our online form today to schedule your free forensic assessment and start strengthening your revenue cycle from the inside out.