If you run a behavioral health or substance use treatment program, you’re already familiar with the ASAM criteria—the American Society of Addiction Medicine’s framework for determining the appropriate level of care for individuals seeking treatment. Clinicians use ASAM to match patients to the right level of care based on their clinical presentation across six dimensions. It’s the clinical standard of the field.
What’s less often discussed is how deeply the ASAM framework intersects with revenue cycle performance. The level of care a patient is placed in, the documentation supporting that placement, and the ongoing justification for continuing care at that level all have direct implications for whether claims get paid, how quickly, and at what rate. Understanding this intersection is essential for any reputable treatment program.
Each Level of Care Has Its Own Billing Complexity
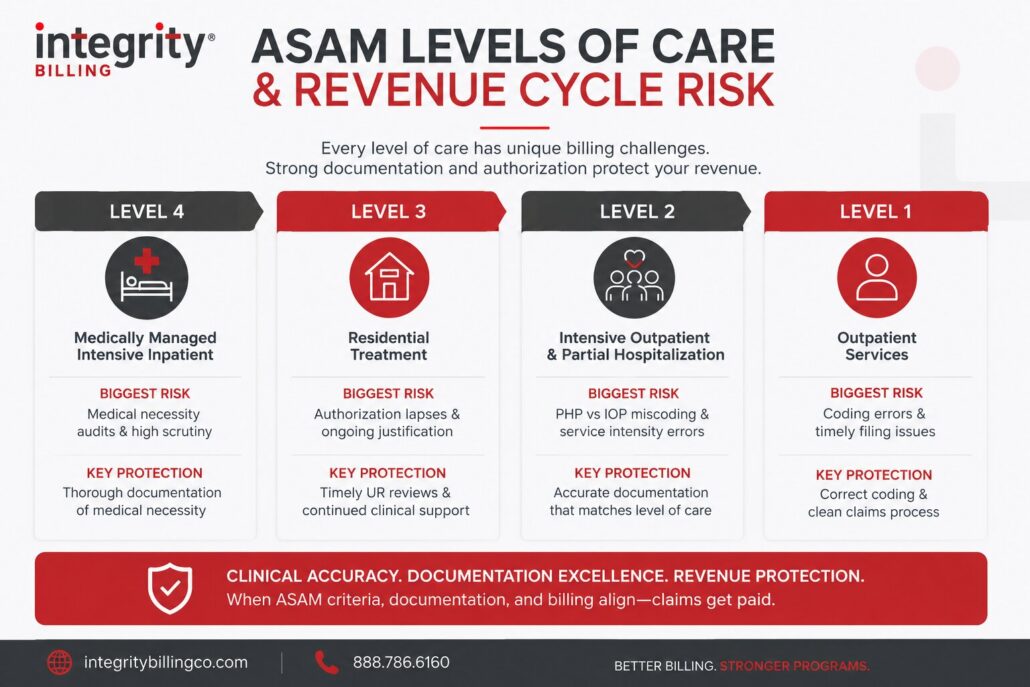
ASAM defines a continuum of care that moves from medically managed intensive inpatient treatment at the highest level of intensity down through outpatient services at the lower end. Within that continuum, each level of care carries its own billing requirements, authorization protocols, documentation standards, and payer-specific rules.
Level 4: Medically Managed Intensive Inpatient
At this level, billing is typically facility-based and involves per diem rates, complex authorization requirements, and close payer scrutiny of medical necessity. Claims at this level are among the most heavily reviewed and the most likely to face audits. Documentation must demonstrate not just that the patient needed inpatient care, but also that they required the level of medical management that distinguishes Level 4 from lower residential placements.
Level 3: Residential Treatment
Residential billing, particularly at 3.5 (clinically managed high-intensity residential) and 3.1 (clinically managed low-intensity residential), is an area where authorization management and medical necessity documentation are critical. Payers require ongoing clinical justification to continue authorizing residential days, and authorization lapses at this level are one of the most common and costly revenue cycle failures in behavioral health.
Level 2: Intensive Outpatient and Partial Hospitalization
PHP and IOP are levels of care where billing and coding precision is particularly important. The distinction between PHP and IOP needs to be clearly reflected in both the documentation and the claim. Payers are attentive to the line between these levels of care, and billing that doesn’t accurately represent the service intensity invites denial.
Level 1: Outpatient Services
Outpatient billing carries its own complexity, particularly around the use of correct procedure codes for individual therapy, group therapy, family sessions, and psychiatric services. At this level, the documentation requirements are less intensive than higher levels of care, but coding accuracy and timely filing remain essential.
Medical Necessity Documentation Has to Match the Level
One of the most important connections between ASAM and revenue cycle performance is documentation. ASAM is not only a clinical tool; it also gives treatment programs a framework for showing medical necessity in a way payers recognize. When a patient is placed at a specific level of care, the clinical record needs to clearly explain why that placement is appropriate and connect the documentation back to the ASAM criteria that support the level of care being billed.
The ASAM framework looks at six key dimensions:
- Intoxication and withdrawal potential
- Biomedical conditions
- Emotional and cognitive conditions
- Readiness to change
- Relapse potential
- Recovery environment
Together, these dimensions help create a defensible clinical picture. They show not only what the patient is struggling with, but also why a particular level of care is medically necessary. If the documentation does not clearly connect the patient’s needs to these criteria, denial management becomes much more difficult because the claim is more vulnerable to medical necessity denials.
Level Transitions Create Revenue Cycle Risk
Patient movement between levels of care is a vulnerable point in the revenue cycle. When a patient steps down from residential treatment to PHP, or from PHP to IOP, several billing requirements need to be handled at the same time. New authorizations must be in place before the transition, billing codes must accurately reflect the new level of care, and documentation must support both the transition itself and the ongoing medical necessity for the new level.
When any of those elements is missing or delayed, claims can quickly fall through the cracks. A patient who transitions from residential treatment to PHP without a new authorization in place may generate denied claims from the first day of the new level of care. A billing team that continues submitting residential codes after the transition creates compliance risk and audit vulnerability. These are common revenue cycle failures when treatment programs manage level-of-care transitions manually or without a clear process.
Utilization Review Is the Bridge Between Clinical and Financial
The connection between ASAM and revenue cycle performance is managed, in large part, through utilization review. A strong UR function ensures that authorizations are obtained before services begin, renewed before they expire, and escalated appropriately when a payer challenges the level of care. It also ensures that the clinical documentation being submitted to payers accurately reflects what ASAM dimensions are driving the placement, making the medical necessity case in the language payers understand.
For treatment programs that manage utilization review internally, the quality of that process has a direct impact on revenue cycle performance at every level of care. For programs that outsource UR or billing support, the partner’s behavioral health expertise matters just as much. A behavioral health billing partner that understands behavioral health-specific utilization review can help protect revenue, while a partner that treats UR as a generic administrative task can allow preventable denials, authorization gaps, and reimbursement delays to slip through.
Connecting Clinical Excellence to Financial Performance
The programs that perform best financially are almost always the ones that recognize clinical quality and revenue cycle performance are not separate priorities. When ASAM placements are clinically sound, documentation is thorough, utilization review is proactive, and billing is accurate at every level of care, the revenue follows.
At Integrity Billing, we work with substance use and behavioral health treatment programs at every level of the ASAM continuum to build revenue cycle processes that reflect clinical realities accurately and protect the revenue those programs have earned.
If your program’s financial performance isn’t keeping pace with the quality of your clinical work, a free forensic billing assessment is the clearest way to find out why. Request yours today by filling out our contact form or calling us at 888-368-7461.