
Running a behavioral health clinic is complex work. Every day, you’re managing staff, supporting patients, and keeping up with ever-changing regulations. Somewhere in the middle of all of that, you’re also expected to keep your behavioral health billing airtight.
The reality is that billing mistakes in behavioral health are incredibly common. Not because teams are careless, but because the system itself is complicated. Payer rules vary, documentation requirements shift, and billing and coding nuances can trip up even experienced organizations.
While billing errors are common, this doesn’t mean they’re harmless. Small oversights quietly drain revenue, invite audits, and create compliance risks that can have serious consequences. Let’s take a closer look at some of the billing mistakes we see most often at Integrity Billing and what you can do to prevent them.
1. Upcoding and Downcoding—Both Are Costly
Upcoding (billing for a higher level of service than was actually provided) is one of the most scrutinized issues in behavioral health billing. In fact, it can even trigger fraud investigations. But downcoding is just as damaging, even if it flies under the radar.
Many clinics consistently undercode their services out of an abundance of caution, leaving revenue on the table every single month. If your clinicians are regularly providing 60-minute therapy sessions but billing for 45-minute codes, you are underpaying yourself for the work you’re actually doing.
The fix isn’t to bill higher—it’s to bill accurately. That starts with documentation that clearly reflects the service delivered and a billing process that matches codes to what’s actually in the record.
2. Poor Documentation That Can’t Support the Claim
This is the root cause of a huge percentage of behavioral health billing problems. A claim is only as strong as the documentation behind it, and payers know this. When documentation is vague, incomplete, or doesn’t clearly support the level of service billed, your practice becomes vulnerable. Sometimes this issue appears immediately at the time of billing; other times it surfaces months later during an audit.
Common documentation gaps we see in behavioral health include:
- Missing or incomplete treatment plan updates
- Progress notes that don’t reflect medical necessity
- Session notes that are templated or copy-pasted without individualization
- Missing signatures, dates, or provider credentials
Strong documentation may seem like just a billing requirement, but it’s actually a form of clinical protection. When your notes clearly tell the story of a patient’s treatment and progress, compliant billing naturally follows.
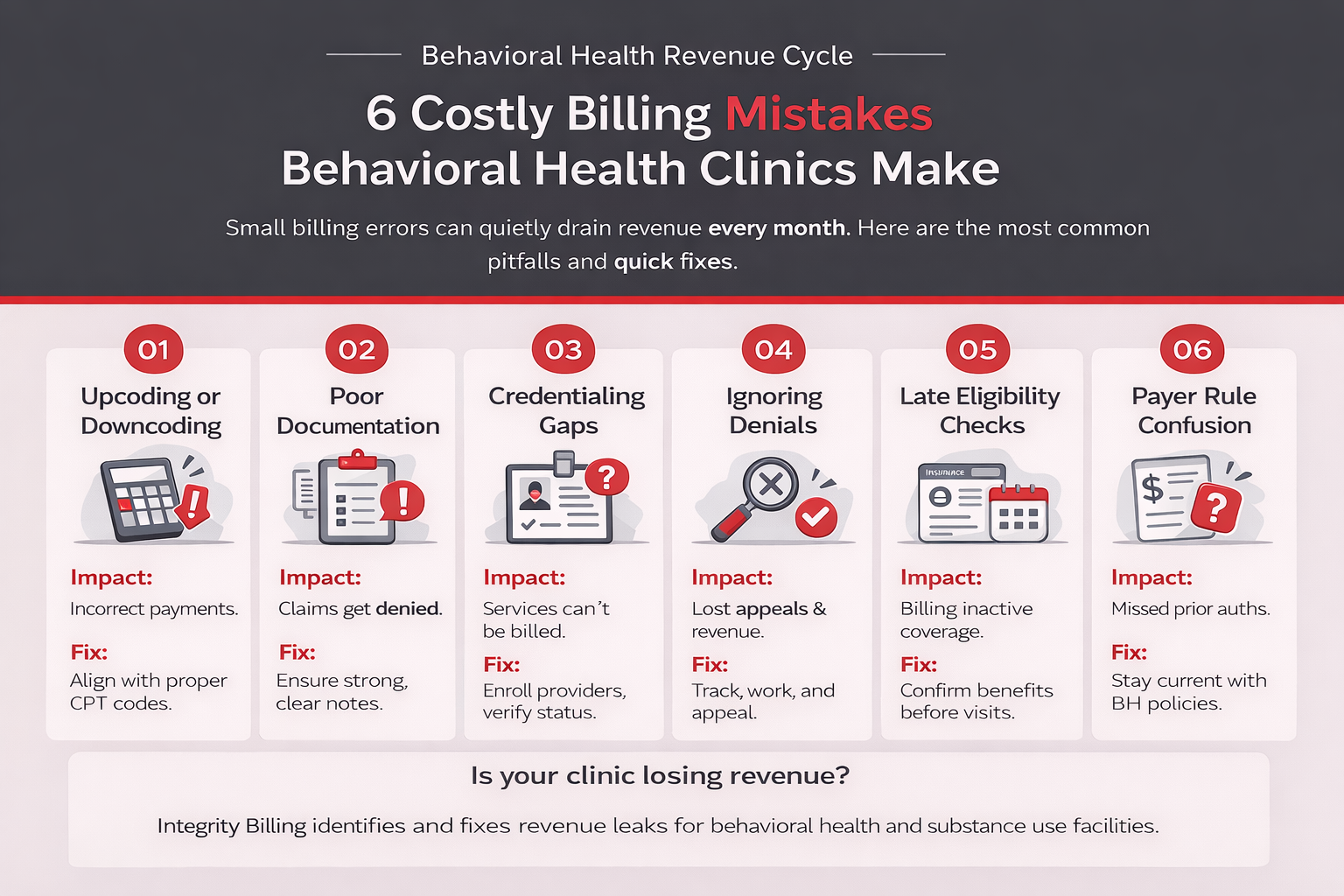
3. Credentialing Gaps and Billing Under the Wrong Provider
Credentialing is the process of verifying and enrolling your providers with insurance payers. It’s also one of the most commonly mismanaged areas in behavioral health billing. Billing for services performed by a provider who has not yet been credentialed with a payer can result in denied claims at best and compliance violations at worst.
This issue often arises with new hires. Let’s say a clinician joins your team and begins seeing patients right away, but the credentialing process with one or more payers is still pending. As a result, claims may be denied, or if they are paid incorrectly, they may later require refunds. Either way, the outcome is the same: lost revenue and increased compliance risk.
Incident-to billing rules can add another layer of complexity in supervisory arrangements. Many behavioral health organizations rely on supervised clinicians, but the rules governing when services can be billed under a supervising provider’s NPI are highly payer-specific and often misunderstood. When these rules are applied incorrectly, claims may be denied or flagged for compliance review.
Is your billing leaving money on the table? A forensic billing assessment from Integrity Billing can identify exactly where your revenue is leaking, from denied claims and undercoding to documentation gaps and credentialing errors. Most clinics are surprised by what we find. Request your free forensic assessment today.
4. Not Following Up on Denied and Rejected Claims
Every behavioral health clinic has a denial rate. The question is whether you’re managing it actively or letting revenue quietly disappear.
Denials and rejections are not the same thing. A rejected claim never made it into the payer’s system due to an error, such as a wrong code, missing information, or eligibility issue. A denied claim was received and reviewed, then not paid. Both require follow-up, and both have deadlines. Miss the timely filing window on a denial, and you lose that revenue permanently.
Many clinics lack a consistent process for tracking, working, and appealing denied claims. The result is a growing pile of unresolved claims that ages out before anyone gets to it. A good billing operation treats every denial as recoverable revenue until proven otherwise.
5. Eligibility Verification Happening Too Late (or Not at All)
Verifying a patient’s insurance benefits before their appointment sounds basic. But in busy behavioral health practices, it often gets skipped, rushed, or done inconsistently. Unfortunately, the downstream consequences can be significant.
Insurance information changes constantly. A patient who was fully covered three months ago may have changed employers, lost coverage, or entered a new plan year with a different deductible structure. If you’re finding out about these changes after services are rendered, you’re either billing a payer who won’t pay or collecting the wrong amount from the patient.
Verification should happen at every appointment, not just at intake. It takes minutes and saves hours of rework.
6. Misunderstanding Behavioral Health-Specific Payer Rules
Behavioral health billing operates within a complex set of payer-specific rules that differ significantly from traditional medical billing. Prior authorization requirements, utilization review processes, session limits, diagnosis-specific coverage rules, telehealth parity laws, and behavioral health carve-outs all create a web of requirements that can vary by payer, by plan, and sometimes even by state.
A billing process that works well for your Blue Cross patients may create problems with Medicaid managed care plans or behavioral health carve-out payers. Staying current with these rules is essentially a full-time job, which is why many organizations benefit from partnering with a billing team that specializes specifically in behavioral health, rather than general medical billing.
The Right Billing Partner Makes All the Difference
You didn’t open a behavioral health clinic to spend your energy untangling billing errors. But those errors have real consequences for your revenue, your compliance posture, and your ability to serve the patients who need you.
At Integrity Billing, we specialize exclusively in behavioral health revenue cycle management. We know the codes, the payers, the documentation requirements, and the compliance landscape. We also know how to help clinics like yours run cleaner, get paid faster, and stop leaving money behind.
Ready to see what’s really happening in your billing? Contact Integrity Billing today at 888-368-7461 for a consultation and let’s take a look together.