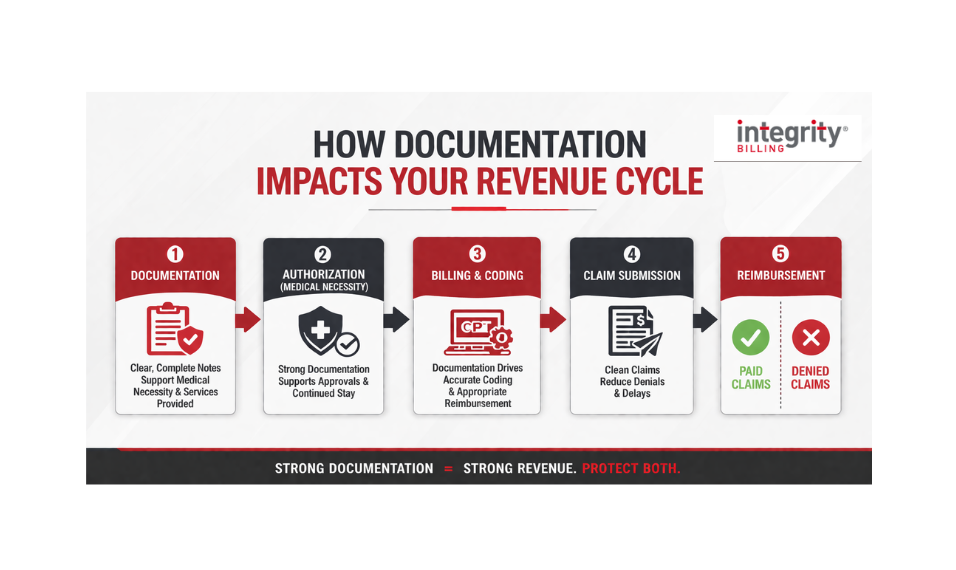
Clinical documentation has a direct impact on your bottom line, yet it often does not get the attention it deserves. Whether you run a residential treatment center, outpatient program, or intensive outpatient program (IOP), the notes your clinicians write every day do far more than track patient progress. They support medical necessity, justify the level of care, and protect the revenue your organization depends on.
When documentation is clear, complete, and aligned with payer expectations, it strengthens your entire revenue cycle. When it falls short, even strong clinical care can lead to delays, denials, and lost reimbursement. Understanding the connection between documentation and behavioral health reimbursement is the first step toward building processes that protect both your patients and your financial health. Let’s take a closer look at how documentation works and why it matters so much.
Documentation Is the Foundation of Every Claim
When it comes to behavioral health billing, insurance companies don’t just pay for what happened in a session—they pay for what was documented about what happened. Every claim you submit is essentially a story. It has characters (the patient, the clinician), a setting (the level of care), a plot (the presenting issues and treatment goals), and evidence (progress notes, assessments, treatment plans). If any part of that story is missing, vague, or inconsistent, you’re giving the payer a reason to deny or reduce your reimbursement.
This is where many behavioral health facilities lose money without realizing it. A clinician might deliver an excellent, medically necessary session, but if the note reads like a checkbox exercise rather than a clinical narrative, the payer has little to justify the payment.
Common documentation gaps that lead to denials:
- Missing medical necessity language. Notes that describe what happened but don’t clearly establish why the level of care was appropriate.
- Vague progress indicators. Generic phrases like “patient engaged in session” without measurable clinical detail.
- Unsigned or late-signed notes. Even a great note can trigger a denial if it wasn’t signed within your payer’s required timeframe.
- Inconsistency between documents. When the treatment plan, progress notes, and discharge summary don’t tell a cohesive story.
- Missing co-signatures. Notes written by unlicensed or provisionally licensed staff that lack required supervisor sign-off.
Medical Necessity: The Heart of Every Authorization
Medical necessity drives behavioral health reimbursement more than anything else. Payers not only want to know what services were provided but also understand why the patient needed them, why they needed them at this particular level of care, and why they continue to need them going forward.
This is especially critical during the utilization review process. When a payer’s UR team reviews a request for continued stay or a new authorization, they are scrutinizing your clinical documentation with one central question in mind: does this documentation support the medical necessity of this level of care?
Your clinical team may know the answer is absolutely yes. But if the documentation doesn’t clearly show this, that authorization can be denied. Partial denials and retrospective denials are another major source of lost revenue. Documentation is almost always the deciding factor in these cases.
Think of it this way: Your clinicians know the patient. Your documentation has to convince someone who’s never met them.
How Billing and Coding Connects Back to Your Notes
Strong documentation doesn’t just support authorization—it directly informs your billing and coding accuracy. The CPT codes your billing team submits need to be supported by what’s in the clinical record. If a clinician provides a 60-minute individual therapy session but the note only documents 30 minutes of clinical content, you’re either under-billing or at risk of an audit if you bill the full time.
Similarly, if your facility provides services that qualify for add-on codes (e.g., crisis intervention, medication management, or specific evidence-based interventions), those services need to be documented in a way that makes the coding defensible. Coders can only work with what they’re given. When documentation is incomplete or inconsistent, even the best billing and coding team is forced to make conservative decisions.
This is also where internal auditing becomes so valuable. Regular documentation audits can reveal patterns that are quietly eating into your reimbursement. Things like services being consistently undercoded, notes that don’t support the billed procedure, or entire service components going unbilled because they weren’t clearly documented.
The Credentialing Connection
Here’s one that often surprises facility leaders: credentialing issues are one of the most common reasons behavioral health claims get denied.
When a provider isn’t properly credentialed with a payer, or when their credentialing has lapsed, every claim they submit can be denied. This is the case even when the documentation is perfect. And here’s the frustrating part: these denials often don’t show up until weeks or months after services were rendered. By then, you’re dealing with a mountain of retroactive denials.
Good documentation practice includes knowing who is signing notes and ensuring that person’s credentials are current and in-network with the payer. Facilities that build a habit of cross-checking service documentation against credentialing status, especially during onboarding of new staff, catch these problems before they become expensive.
Utilization Review: Where Documentation Gets Put to the Test
Think of utilization review as the moment your documentation has to stand on its own without you in the room. The UR reviewer isn’t talking to your clinicians but rather reading what those clinicians wrote. And they’re comparing it against very specific clinical criteria to decide whether to approve continued care.
Facilities that consistently pass UR tend to share a few habits: their notes connect the dots between the patient’s presenting symptoms, the treatment being provided, and the patient’s response to that treatment. They document not just progress but also barriers to progress, risks that justify continued care, and a clear clinical rationale for why step-down to a lower level isn’t yet appropriate.
This kind of documentation takes practice and intention. It does not happen by accident.
A Culture Shift, Not Just a Compliance Mandate
One of the most important things you can do as a facility leader is help your clinical team understand that documentation quality is about sustainability. When your facility gets paid accurately for the care it provides, you can hire more staff, maintain quality programming, and serve more patients. When documentation gaps lead to chronic underpayment, something eventually gives.
At Integrity Billing, we work exclusively in the behavioral health space because we believe the work you do deserves a billing partner who truly gets it. If you’re ready to take a hard look at whether your documentation is supporting or undermining your reimbursement, we’d love to help.
Is your documentation costing you revenue? Our forensic billing assessment takes a deep dive into your claims, documentation patterns, and denial history to identify exactly where your revenue is slipping through the cracks—and what to do about it. Request your free forensic billing assessment today.