
Getting paid for the care you provide is essential to running a successful behavioral health facility but it’s rarely straightforward. Between insurance verification, authorization requirements, documentation standards, billing and coding rules, and denial management, your revenue cycle is complex—even by healthcare standards.
And if you’re like many clinic administrators and owners, you may not have full visibility into every step of that process. Do you know where the most common breakdowns occur? Or how each stage impacts the next? These gaps in visibility are often where revenue quietly slips through the cracks.
To help you better understand how the behavioral health revenue cycle works, here’s a clear, plain-language walkthrough—from the moment a patient first contacts your clinic to the moment payment hits your account. Because when you can see the full picture, you’re in a much stronger position to improve it.
Stage 1: Patient Intake and Insurance Verification
Everything starts before the first session. The intake process sets the foundation for whether a claim will succeed or fail weeks later. This is also where a surprising number of preventable problems start.
At intake, you’re collecting demographic information, insurance details, and consent documentation. But the critical piece is insurance verification, which refers to confirming the patient’s active coverage, benefits for behavioral health services, deductible and copay amounts, and any plan-specific requirements like referrals or network restrictions.
This needs to happen before every appointment, not just at the first visit. Insurance changes constantly. A patient who had excellent coverage in January may be on a different plan in April with different benefits, a new deductible, or a different payer altogether. Finding out at the claim stage that the patient’s policy changed months ago is something you can avoid entirely.
Stage 2: Credentialing
Credentialing is the process of enrolling your providers with insurance payers so services can be billed and reimbursed. Without proper credentialing, providers simply can’t bill a payer for the care they deliver. And if credentialing lapses or includes outdated information, it can lead to denied claims and potential compliance risks.
What often surprises organizations is just how long credentialing can take—typically 90 to 120 days or more. The longer it takes to start the process, the longer your revenue is delayed.
This becomes especially critical for behavioral health organizations that frequently hire new clinicians or expand into new locations. Credentialing quickly shifts from a one-time task to an ongoing operational challenge. Tracking expiration dates, managing payer-specific re-credentialing requirements, and monitoring pending enrollments is a job in itself—and one that can easily fall through the cracks in a busy clinic.
Stage 3: Authorization and Utilization Review
Many behavioral health services require prior authorization before they’re covered, and this is where utilization review enters the picture. Utilization review (UR) is the process by which payers assess whether the services requested are medically necessary and appropriate for the level of care being provided.
For services like PHP (Partial Hospitalization Programs) and IOP (Intensive Outpatient Programs), utilization review is typically ongoing. Payers conduct concurrent reviews throughout the treatment period, and if the documentation doesn’t clearly demonstrate continued medical necessity, they’ll stop authorizing sessions.
Strong utilization review management requires clinical documentation that is consistently specific, progress-focused, and clearly tied to the treatment plan. It also requires someone (a team member or billing partner) to actively track authorization windows, submit concurrent review requests on time, and follow up when reviews are delayed or challenged.
Is your revenue cycle losing money you don’t know about?
A forensic billing assessment from Integrity Billing examines your entire revenue cycle, from credentialing gaps and authorization tracking to billing and coding patterns and denial trends. Let us identify exactly where your revenue is leaking. Request your free forensic billing assessment today to get started.
Stage 4: Clinical Documentation
Every claim that goes out the door is only as strong as the documentation that supports it. Payers don’t reimburse the service but rather the documented service. If the note doesn’t support the level of care billed, the claim is vulnerable.
In behavioral health specifically, documentation failures tend to follow recognizable patterns: progress notes that are templated or copy-pasted without individualization, treatment plans that haven’t been updated to reflect the patient’s current status, or notes that describe what happened in the session but don’t clearly establish medical necessity. Missing credentials or signatures are also common.
While training can help, the most important fix is to build documentation expectations into your clinical workflow so that the right information is captured consistently, every time. When your notes tell a clear story about why this patient needs this level of care, billing follows naturally.
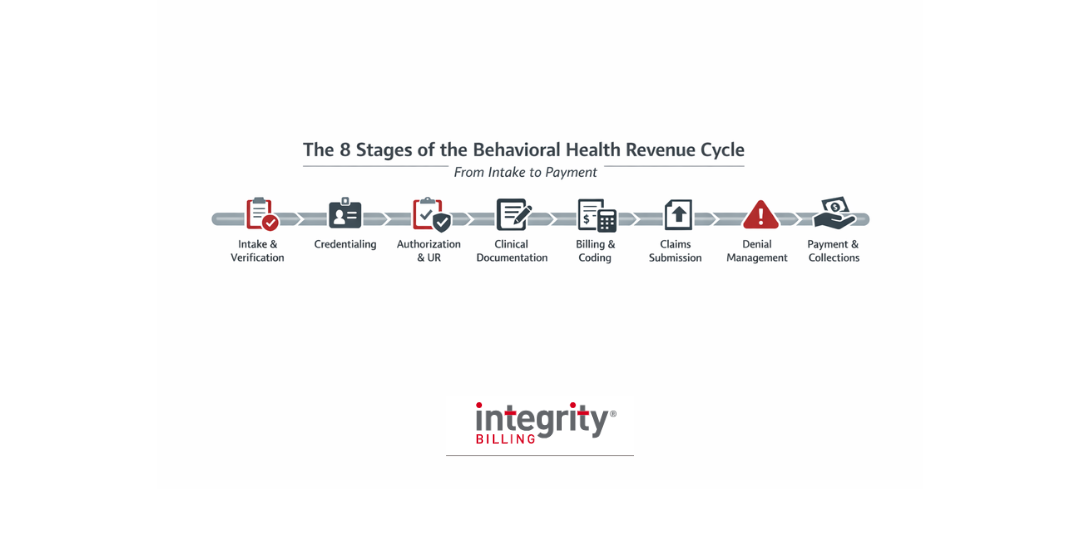
Stage 5: Billing and Coding
This is where all of the upstream work—verification, credentialing, authorization, documentation—comes together into an actual claim. Behavioral health billing and coding is its own specialized discipline, and you don’t want to underestimate its complexity.
The code sets used in behavioral health (e.g., CPT codes for therapy services, E&M codes for psychiatric evaluation and management, HCPCS codes for certain programs) require precise application. For example, the difference between a correctly coded 60-minute psychotherapy session and a 45-minute code is money left on the table.
Modifier usage adds another layer. Telehealth modifiers, place-of-service codes, and program-specific codes like those used for PHP and IOP all have payer-specific rules that vary and change. What’s correct billing for one payer may generate a denial for another. Timing also matters, as clean claims submitted on time have better reimbursement rates.
Stage 6: Claims Submission and Adjudication
Once a claim is coded and submitted, it enters the payer’s adjudication process. The payer reviews the claim against the patient’s benefits, your contract terms, and their internal policies. They then either pay the claim, partially pay it, or deny it.
The goal at this stage is to submit clean claims, which are claims that contain accurate information, pass all payer edits, and are submitted within timely filing windows. Electronic claim submission with real-time eligibility checks and claim scrubbing dramatically improves clean claim rates and reduces the volume of rejections that need to be worked before they even reach the payer.
Tracking claim status actively allows your billing team to intervene early if a claim is stuck, rejected, or heading toward a denial. In many cases, a quick correction at the right time makes all the difference in getting paid or not.
Stage 7: Denial Management and Appeals
Denials are a fact of life in behavioral health billing. Every clinic has a denial rate. What separates high-performing billing operations from struggling ones isn’t the absence of denials but rather how systematically and quickly they’re worked.
Denials need to be reviewed, categorized by root cause, and addressed within the payer’s appeal window. Miss that window and the revenue is gone permanently. Work denials without understanding the pattern behind them and you’re solving the same problem over and over again at the claim level instead of fixing it upstream.
A strong denial management process identifies root causes. Is it a credentialing issue? A documentation gap? A coding pattern? An authorization miss? It then feeds that information back into the revenue cycle so the same errors stop repeating.
Stage 8: Payment Posting and Patient Collections
When payment does arrive, it must be posted accurately. That means matching it to the correct claim, applying it to the appropriate patient account, and reconciling it against the remittance advice. Even small errors in payment posting can create accounts receivable issues that compound over time, making it difficult to understand what’s truly outstanding versus what has already been collected.
Once insurance has paid its portion, any remaining balance shifts to patient responsibility. At that point, the process moves into patient collections—issuing accurate statements, following up on unpaid balances, and managing payment plans when needed. In behavioral health, where the therapeutic relationship is especially important, these communications must be handled with care, clarity, and sensitivity.
You’ve Built Something Worth Getting Paid For—Let’s Make Sure You Are
The behavioral health revenue cycle has a lot of moving parts, and a problem at any stage affects everything downstream. Most organizations don’t have a clear picture of where their revenue is slipping until they take a hard look, and what they find is usually more than they expected.
At Integrity Billing, we specialize exclusively in behavioral health billing. We know the payers, the codes, the documentation standards, the credentialing landscape, and the authorization requirements. We’ve seen virtually every revenue cycle problem that exists in behavioral health and we know how to fix them.
Contact Integrity Billing today at 888-368-7461 to learn more about how we can support your revenue cycle.