Clinical documentation and financial performance may seem like two separate worlds, with one belonging to clinicians and the other to the billing team. In reality, they are closely connected. The quality, completeness, and clarity of the documentation created during patient care can have a major impact on a behavioral health practice’s financial health.
When documentation is strong, billing runs cleaner, denials decrease, and revenue becomes more predictable. The practice is also better prepared to withstand payer scrutiny. When documentation is incomplete, vague, or inconsistent, the financial consequences can show up quickly through delayed payments, denied claims, and missed reimbursement opportunities.
Understanding this connection is the first step toward improving behavioral health billing performance, reducing preventable denials, and building a revenue cycle that better supports the clinical work happening every day.
Documentation Is the Foundation of Every Claim
Every claim submitted to an insurance payer is built on documentation. The billing code, the level of service, and the medical necessity justification all have to be supported by what was written in the clinical record. If the documentation does not clearly support what was billed, the payer has every reason to deny, downcode, or scrutinize the claim.
This is where many behavioral health practices quietly lose money without fully understanding why. Let’s say a clinician delivers a high-quality, medically necessary session, and the billing team submits the claim at the appropriate level. However, the documentation doesn’t paint a complete enough picture. It doesn’t capture the clinical complexity, the patient’s functional impairment, or the specific interventions used in enough detail to satisfy the payer’s criteria.
As a result, the claim comes back denied or downgraded, and revenue that should have been collected simply isn’t. The care was real, but the documentation didn’t do it justice.
What “Better” Documentation Looks Like
Improving clinical documentation is not about writing more — it’s about writing smarter. The goal is to tell a clear, complete clinical story: one that establishes medical necessity, supports the level of service billed, demonstrates clinical reasoning, and tracks the patient’s progress or lack thereof over time.
In practical terms, stronger documentation typically includes:
- A clear description of the patient’s presenting symptoms and functional impairment, not just a diagnosis code
- Specific treatment interventions documented by name, not generic references to “counseling” or “support”
- The patient’s response to treatment and any changes in clinical status
- A documented treatment plan that is individualized, measurable, and regularly updated
- Clear medical necessity language that ties the level of care to the patient’s clinical needs
- Progress notes that reflect what actually happened in the session, not templated language copied from a previous visit
When documentation consistently hits these marks, the billing team has everything it needs to submit clean claims, and payers have far less basis for denial.
The Denial Connection
Claim denials are expensive. Not only in lost revenue but also in the staff time required to appeal, resubmit, and follow up. In behavioral health, documentation gaps are one of the leading causes of denial.
When a payer denies a claim for lack of medical necessity or insufficient documentation, they are essentially saying: the record you provided doesn’t tell me enough to justify paying for this service. The fix is almost never a billing issue. It’s a documentation issue that needs to be addressed upstream, at the point of care.
Practices that invest in documentation training, clinical supervision that includes a documentation quality component, and regular audits of their records against payer criteria often see measurable reductions in denial rates. That stronger approach to denial management can lead directly to improved cash flow and a healthier revenue cycle.
Free Forensic Assessment
Not sure how your documentation is holding up against payer standards? Integrity Billing offers a complimentary forensic assessment to identify documentation gaps, billing vulnerabilities, and revenue opportunities your practice may be missing. Reach out today to schedule yours.
Documentation Quality and Utilization Review
The stakes around documentation become even higher when authorizations are involved. Payers conducting utilization review are making coverage decisions based almost entirely on the clinical record. A well-documented record that clearly establishes ongoing medical necessity gives reviewers what they need to approve continued care.
On the other hand, a record that relies on vague language, templated notes, or missing progress documentation gives reviewers a reason to question whether continued treatment is justified. Practices that see high rates of authorization denials or concurrent review challenges often find that documentation quality is the root cause, not the clinical necessity of the care itself.
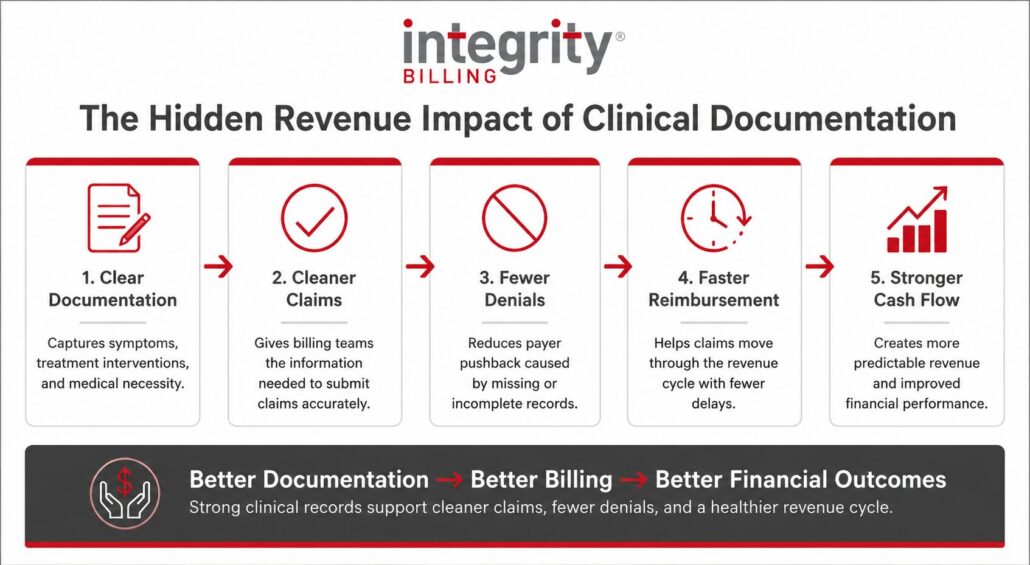
Connecting Documentation to the Bottom Line
The financial case for better clinical documentation is simple: better documentation leads to cleaner claims, fewer denials, and more predictable revenue. Over time, the difference between strong documentation habits and recurring documentation gaps can have a significant impact on a behavioral health practice’s financial performance.
Strong clinical documentation can help practices:
- Submit cleaner claims: Complete, accurate documentation gives the billing team what they need to code and submit claims correctly the first time.
- Reduce preventable denials: When medical necessity, level of care, and services provided are clearly supported in the record, claims are less vulnerable to payer pushback.
- Improve revenue predictability: Fewer denials and delays help revenue move more consistently through the billing cycle.
- Strengthen audit readiness: Well-documented records make it easier to respond to payer reviews, audits, and documentation requests.
- Lower compliance risk: Clear, consistent documentation helps protect the practice by supporting the clinical and billing decisions being made.
At Integrity Billing, we help behavioral health practices connect clinical excellence with financial performance. Our team understands both sides of the revenue cycle and works with providers to improve documentation practices in ways that support cleaner billing, stronger compliance, and measurable results.
Ready to Strengthen Your Practice’s Financial Performance?
Better documentation leads to better outcomes, clinically and financially. If you’re ready to find out where your practice stands and what’s possible, Integrity Billing is here to help. Contact us today at 888-368-7461 or fill out our online form to learn more about how we partner with behavioral health practices to improve documentation, reduce denials, and build stronger revenue cycles from the ground up.